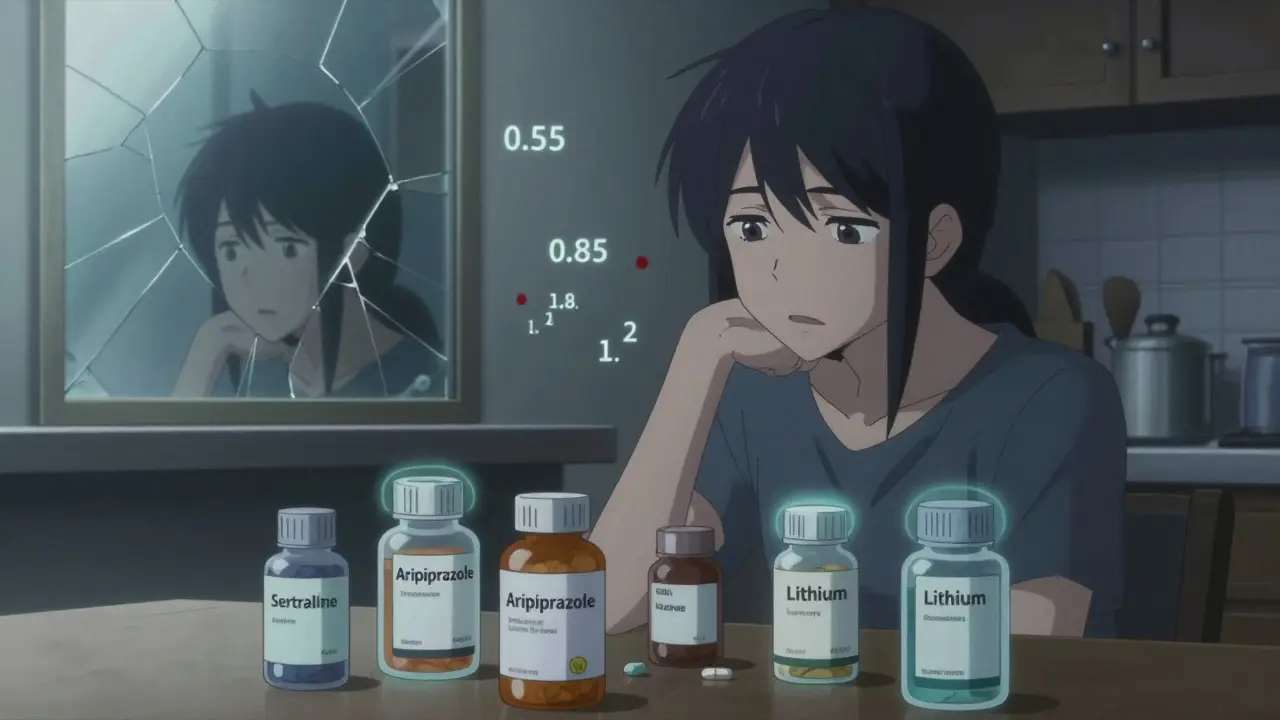
When a single psychiatric medication doesn’t do the job, doctors often turn to combinations. It’s not uncommon for someone with treatment-resistant depression to be on an SSRI like sertraline plus a low dose of aripiprazole. Or someone with bipolar disorder might be taking lithium along with lamotrigine. These combinations aren’t random-they’re backed by years of research and clinical trials. But here’s the catch: when you switch from a brand-name drug to a generic version, things can go sideways-fast.
Why Combine Medications in the First Place?
Monotherapy works for some. But for many, it doesn’t. The STAR*D trial, one of the largest depression studies ever done, found that nearly 40% of people didn’t respond to their first antidepressant. That’s why combinations became standard practice. Adding a low-dose antipsychotic like aripiprazole to an SSRI can push remission rates up by 15-20%. Symbyax, a fixed-dose combo of fluoxetine and olanzapine, was approved in 2003 specifically for people who hadn’t improved with antidepressants alone. These aren’t last-resort options anymore-they’re part of the toolkit.Other common combinations include adding buspirone to an SSRI for lingering anxiety, or pairing bupropion with an SSRI to fix sexual side effects. The science behind them is solid. But that doesn’t mean they’re easy to manage.
The Generic Switch Problem
The FDA says generics are the same as brand-name drugs. They have to contain the same active ingredient and be within 80-125% bioequivalence. Sounds fair, right? Not when you’re dealing with psychiatric meds.That 45% window between low and high bioavailability is huge when your brain is finely tuned. A 2019 study of nearly 28,500 patients found that switching from brand to generic SSRIs led to a 22.3% higher chance of treatment failure. That’s not a small bump. That’s people relapsing, crashing, ending up back in the ER.
Lithium is the worst offender. Its therapeutic range is razor-thin: 0.6 to 1.2 mmol/L. Go a little low, and depression returns. Go a little high, and you get tremors, confusion, even kidney damage. A 2018 case series from the University of British Columbia showed three bipolar patients going into mania within two weeks of switching from Eskalith to a generic lithium. Their blood levels dropped from 0.85 to 0.55-despite the same daily dose. That’s not a glitch. That’s a systemic flaw.
Where the System Breaks Down
Some generics are worse than others. Generic bupropion XL, for example, has been flagged by the FDA since 2012. Over 130 adverse event reports linked it to breakthrough anxiety, mood swings, and relapse. The issue? Different manufacturers use different bead-release technologies. One might release the drug too fast. Another too slow. The result? You’re not getting the same steady level your brain got used to.Venlafaxine ER (Effexor XR) is another problem child. Its effectiveness relies on a precise 2:1 ratio of serotonin to norepinephrine reuptake inhibition. Generic versions? Some use different bead systems. That ratio gets thrown off. And when you’re on a combo-say, venlafaxine plus buspirone-that imbalance can destabilize the whole system.
Even something as simple as switching from one generic manufacturer to another-say, from Mylan to Aurobindo-can cause trouble. A 2021 case report showed a patient on lithium and carbamazepine developed toxic levels. The fix? Going back to the original generic brand. The manufacturer mattered more than the drug name.
What Patients Are Saying
Online forums don’t lie. On Reddit’s r/depression, a top post from May 2023 titled “Generic switch ruined my carefully balanced med cocktail” has over 1,200 upvotes and nearly 300 comments. People describe sudden panic attacks, obsessive thoughts returning, or Zoloft suddenly “not working” after a generic switch. On PatientsLikeMe, nearly 39% of people on combination therapy reported worse symptoms after switching to generics-more than triple the rate of those on single meds.One RN shared a case on GoodRx: a patient on Prozac and Seroquel developed akathisia-a terrifying, restless agitation-within 10 days of switching to generic fluoxetine. They ended up hospitalized. That’s not anecdotal noise. That’s clinical reality.
There are exceptions. Some people switch just fine. A Drugs.com reviewer said their generic Effexor XR actually reduced nausea. But those are the outliers. The pattern is clear: when you’re on more than one psych med, the risk of something going wrong spikes.
How to Protect Yourself
If you’re on a combination, don’t assume your pharmacist’s automatic substitution is safe. Here’s what works:- Know your meds. Write down the exact brand and generic name, dosage, and manufacturer. If your prescription says “venlafaxine ER,” ask: Which one? Teva? Mylan? Aurobindo?
- Don’t switch during a crisis. Wait until you’re stable. Switching during a depressive episode or manic phase is asking for trouble.
- Get baseline scores. Ask your doctor to use a tool like the MADRS (Montgomery-Åsberg Depression Rating Scale) before any switch. That way, you have a measurable baseline to compare against.
- Follow up fast. Schedule a check-in within 7-10 days after any change. Watch for subtle signs: trouble sleeping, increased anxiety, irritability, brain fog. These aren’t “just stress.” They’re red flags.
- Track your levels. If you’re on lithium, valproate, or carbamazepine, ask for a blood test 7-14 days after a generic switch. That’s not optional. That’s essential.
The University of Toronto even created a risk-assessment tool. Add up points: 3 for narrow therapeutic index, 2 for multiple meds, 4 if you’ve had bad reactions before. Score 6 or higher? Your doctor needs to be notified. No exceptions.
The Bigger Picture
The generic psych med market is huge-$18.7 billion in 2022. Insurance companies push for it because it saves money. But the cost isn’t just financial. In 2022, the FDA recorded over 4,800 adverse events tied to generic psychotropic substitutions. That’s a 29% jump from 2020.Some states are catching on. California’s AB 1477, effective January 2023, requires pharmacists to notify prescribers before switching generics in patients on multiple psych meds. Michigan saw a 22% drop in ER visits after passing a similar law.
And now, the FDA is moving. In May 2023, they proposed tighter bioequivalence standards-90-111%-for extended-release psychiatric drugs used in combinations. That’s a big deal. It’s the first time regulators are admitting the current 80-125% range is too loose for these drugs.
Authorized generics-brand-name drugs sold without the brand name-are another option. Symbyax’s authorized generic, launched in 2022, gives you the exact same formulation at a lower price. Ask your doctor if it’s available.
What’s Next?
The future isn’t just about generics. It’s about personalization. Experts predict pharmacogenetic testing-checking your genes to see how you metabolize drugs-will guide which generic you get by 2030. That could cut adverse reactions by 60%.For now, the message is clear: psychiatric medication combinations are powerful tools. But they’re not interchangeable. The same pill, from a different manufacturer, can feel like a different drug. Your brain doesn’t care about the label. It cares about the dose, the timing, the release. And when those change, your stability can vanish.
Don’t let cost savings cost you your mental health. Ask questions. Demand monitoring. Keep records. Your life isn’t a cost-cutting experiment.
Are generic psychiatric medications always safe?
No. While generics are generally safe for many medications, psychiatric drugs-especially those used in combinations-can be highly sensitive to small changes in absorption. For drugs with narrow therapeutic windows like lithium, valproate, or extended-release antidepressants, even minor bioequivalence differences can lead to relapse, mania, or severe side effects. Studies show a 22% higher rate of treatment failure after switching to generics in some cases.
Which psychiatric generics are most likely to cause problems?
Generic bupropion XL, venlafaxine ER, lithium carbonate, lamotrigine, and carbamazepine are the most problematic. Bupropion XL has inconsistent release profiles, leading to mood swings. Venlafaxine ER generics vary in bead technology, altering the serotonin-norepinephrine balance. Lithium’s narrow range means small changes in absorption can trigger mania or toxicity. Lamotrigine and carbamazepine also have variable bioavailability between manufacturers.
Can I switch generics without telling my doctor?
Absolutely not. Even if your pharmacist switches your prescription automatically, you should be notified. For combination therapy, any change in formulation should be discussed with your prescriber first. Some states now require pharmacists to inform doctors before switching psych meds in patients on multiple drugs. Always confirm the manufacturer and lot number with your pharmacy.
How do I know if my generic is causing problems?
Watch for subtle changes: increased anxiety, insomnia, irritability, brain fog, or return of old symptoms. If you feel “off” after a switch-even if you can’t pinpoint why-it’s likely related. Track your symptoms daily. If you’re on lithium or similar drugs, request a blood test within 7-10 days. Don’t wait for a crisis. Early detection saves you from hospitalization.
What’s the difference between a generic and an authorized generic?
A regular generic is made by a different company and may have different fillers or release mechanisms. An authorized generic is made by the original brand-name manufacturer but sold under a generic label. For example, the authorized generic of Symbyax is made by Eli Lilly-the same exact formulation, just cheaper. Authorized generics eliminate the variability risk and are often the safest choice for combination therapy.
Should I avoid generics entirely if I’m on multiple psychiatric meds?
Not necessarily, but proceed with extreme caution. If you’re stable on a brand-name combo, stay on it. If you must switch, choose an authorized generic or stick with the same manufacturer. Always get blood levels checked for narrow-window drugs. Never accept an automatic substitution without your doctor’s approval. Your mental health isn’t a commodity to be swapped for savings.
phara don
February 2, 2026 AT 07:48So wait-generic bupropion XL can mess with your mood just because of bead tech? That’s wild. I switched last year and thought I was just stressed. Turns out my brain was getting hit with a drug bomb every morning. 🤯
Ellie Norris
February 4, 2026 AT 02:51oh my gosh yes!! i was on lithium and switched generics and went into a full manic episode within 10 days-no joke. my doc was like 'huh, weird' but i was like 'no, this is not weird, this is a medical emergency'. blood levels dropped from 0.8 to 0.5 and i was singing show tunes at 3am. 🙃 please, please, please get tested after a switch!!
Marc Durocher
February 4, 2026 AT 21:08Let’s be real-the system is designed to save money, not keep people from screaming into their pillows at 2 a.m. I’ve seen friends go from stable to suicidal after a generic switch. And no one bats an eye because ‘it’s the same drug.’
Same drug? My cat’s litter box is the same material as my couch, but I don’t sit on it. 🤷♂️
larry keenan
February 6, 2026 AT 19:50The bioequivalence window of 80–125% is statistically acceptable for most pharmacokinetic models, yet psychiatric medications operate within a neurochemical equilibrium that is highly nonlinear and individualized. The assumption of therapeutic interchangeability ignores the pharmacodynamic variability inherent in CNS-active compounds, particularly those with narrow therapeutic indices.
Furthermore, the FDA’s adverse event reporting system is underutilized and lacks granular manufacturer-level tracking. This represents a critical gap in post-marketing surveillance for polypharmacy regimens.
Nick Flake
February 8, 2026 AT 02:30MY BRAIN IS NOT A PHARMACY SHELF.
Every time someone says ‘it’s just a generic,’ I hear a CEO laughing while counting cash while someone’s kid has their first panic attack in 6 months because their fluoxetine beads decided to dump all at once.
We treat cancer drugs like sacred artifacts. Why the hell are we treating depression meds like discount laundry detergent?
😭💔 #MyMedsAreNotAMysteryBox
Chinmoy Kumar
February 9, 2026 AT 12:43i am from india and here generics are all we have, but i agree-some feel totally different. i switched from one brand of lamotrigine to another and got this weird floating feeling like my thoughts were underwater. took me 3 weeks to notice it was the med. my doctor didn’t even know the maker changed.
maybe we need a global database? like ‘this generic from x company = bad for y condition’? just a thought 😊
Vatsal Srivastava
February 10, 2026 AT 00:44People are overreacting. If your brain can’t handle a 15% variance in absorption you probably shouldn’t be on psych meds at all. Just take the damn generic and stop whining. Also, your ‘research’ is mostly Reddit posts. LOL
Brittany Marioni
February 11, 2026 AT 08:56PLEASE-PLEASE-PLEASE-ask your pharmacist for the manufacturer name BEFORE they fill it! Write it down! Take a photo of the pill! Keep a log! Your stability is worth more than a $3 copay! I’ve seen too many people lose their minds over this-and I’m not even a doctor, I’m just someone who lost 8 months of progress because someone thought ‘it’s the same thing.’
Don’t be the next statistic.
Love you all.
Stay stable.
-Brittany
Akhona Myeki
February 12, 2026 AT 23:53As a South African psychiatrist with 22 years of experience, I must emphasize that the American obsession with brand-name drugs is a product of pharmaceutical marketing and consumer delusion. In our public health system, generics are the norm-and we have lower relapse rates than the U.S. because we monitor blood levels religiously. Your problem isn’t the generic. It’s the lack of clinical oversight. Fix that, not the pill.