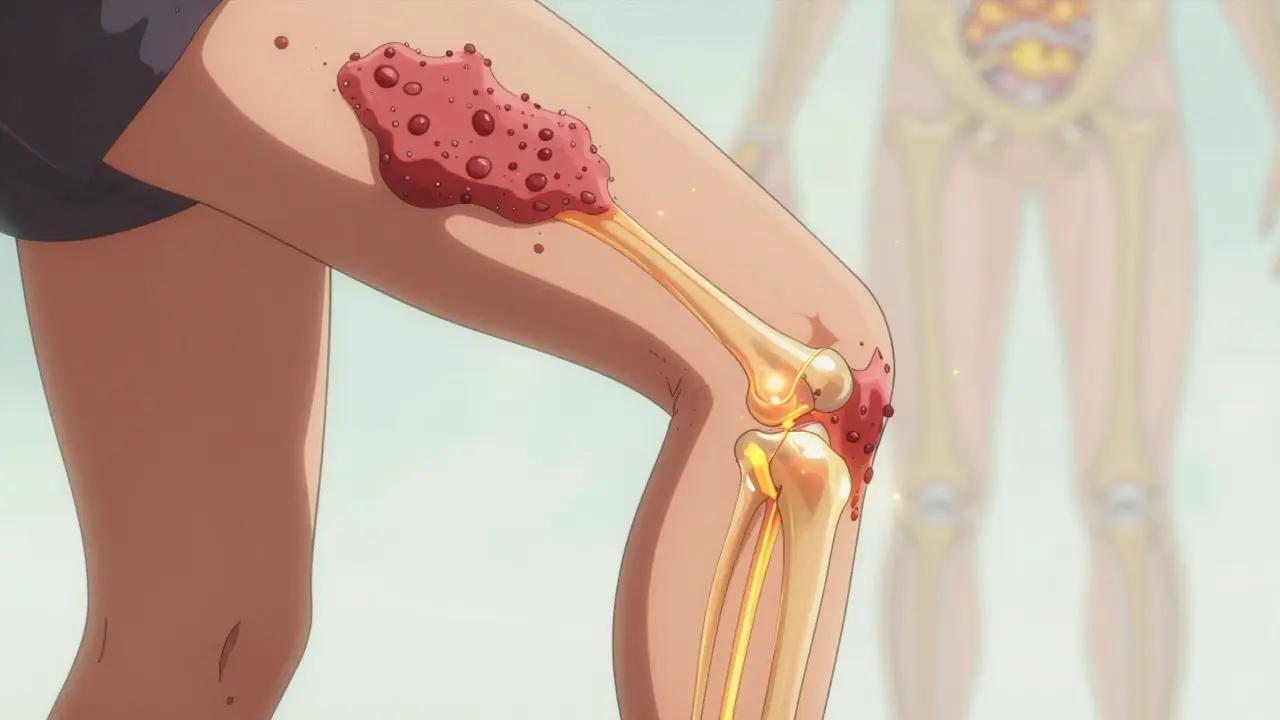
When you think of psoriasis, you probably picture red, scaly patches on your elbows or scalp. But for nearly one in three people with psoriasis, the problem doesn’t stop at the skin. Something deeper is happening - your immune system is attacking your joints too. This is psoriatic arthritis, and it’s not just a side effect. It’s a full-blown autoimmune disease that links skin inflammation to joint destruction.
It Starts in the Skin, But It Doesn’t Stay There
Psoriasis usually shows up years before the joints get involved. On average, people develop skin symptoms 5 to 10 years before joint pain begins. But here’s the twist: in about 15% of cases, the joint pain comes first. That’s why so many people go undiagnosed for years. They see a dermatologist for their skin, then a rheumatologist for their knees - and no one connects the dots. The real clue? Nail changes. If you have pitting, thickening, or lifting of your fingernails or toenails - especially if you also have psoriasis - your risk of psoriatic arthritis jumps dramatically. In fact, 80% of people with psoriatic arthritis have nail changes. For many, these nail problems are the first warning sign.The Five Faces of Psoriatic Arthritis
This isn’t one disease. It’s five different patterns of joint damage, each with its own signature.- Asymmetric oligoarthritis - the most common type - hits fewer than five joints, but not the same ones on both sides. Think: left knee, right wrist. It’s unpredictable and often mistaken for injury or wear and tear.
- Symmetric polyarthritis - affects five or more joints, often on both sides. It looks a lot like rheumatoid arthritis, but without the same antibodies. The key difference? PsA doesn’t usually cause the same level of joint erosion early on.
- Distal interphalangeal predominant (DIP) - this one targets the joints closest to your nails. If your pinky fingers or toes hurt where the nail meets the skin, and you have nail pitting, this is likely your pattern.
- Spondylarthritis - it attacks your spine. Lower back pain that’s worse in the morning and improves with movement? That’s not just aging. It’s inflammation in your sacroiliac joints. Men are more likely to get this form.
- Arthritis mutilans - the rarest and most destructive. It eats away at bone, causing fingers and toes to shorten and twist. Think "opera glass hand" - where you can see through the gaps between the bones. It affects less than 5% of people, but it’s devastating.
What Makes It Different From Other Arthritis?
Osteoarthritis? That’s wear and tear. Your cartilage breaks down over time. No inflammation. No immune system involvement. Just friction. Rheumatoid arthritis? It’s autoimmune too - but it attacks symmetrically. Both wrists. Both ankles. Always. And it’s full of rheumatoid factor in blood tests. Psoriatic arthritis? That test is negative. Always. The real giveaway? Two signs that rarely show up together unless it’s PsA:- Dactylitis - swollen fingers or toes that look like sausages. It’s not just the joint. It’s the whole digit. Tendons, ligaments, and joint lining all inflamed at once. About half of PsA patients have this.
- Enthesitis - inflammation where tendons or ligaments attach to bone. Think: heel pain (Achilles tendon) or bottom-of-the-foot pain (plantar fascia). It’s not plantar fasciitis. It’s PsA.
Why Diagnosis Takes So Long
The average person waits 2 to 5 years to get diagnosed. Why?- Doctors don’t look for it. A dermatologist sees skin. A primary care doc sees "arthritis." No one connects the dots.
- Early symptoms are vague. Stiffness in the morning. Fatigue. Sore heels. People chalk it up to aging, overtraining, or stress.
- There’s no single blood test. No magic marker. Diagnosis relies on pattern recognition - skin, nails, joints, imaging.
Triggers That Make It Worse
Psoriatic arthritis doesn’t come out of nowhere. Something sets it off.- Stress - cited by 85% of patients. Emotional pressure, job loss, grief - all can trigger flares.
- Infections - especially strep throat. The immune system gets overworked and starts attacking your own joints.
- Cold weather - 57% of patients report worse symptoms in winter. Likely due to reduced circulation and increased joint stiffness.
- Obesity - carrying extra weight doesn’t just strain joints. Fat tissue produces inflammatory chemicals that fuel PsA. People with a BMI over 30 are more than twice as likely to develop it.
- Joint trauma - if you twisted your ankle or had a car accident, the joint that got hurt is 4 times more likely to develop PsA there.
Treatment: It’s Not One-Size-Fits-All
The goal isn’t just to reduce pain. It’s to stop joint damage before it’s permanent.- DMARDs like methotrexate are still first-line for many. They work slowly but can slow progression.
- TNF inhibitors - drugs like adalimumab or etanercept - cut inflammation fast. 65% of patients reach minimal disease activity within 6 months.
- IL-17 and IL-23 inhibitors - newer drugs like secukinumab or guselkumab - target specific parts of the immune system. In the FUTURE 7 trial, guselkumab gave 64% of patients a 50% improvement in symptoms at 24 weeks.
When You Need More Than One Doctor
Psoriatic arthritis isn’t a dermatology problem or a rheumatology problem. It’s both. Studies show that 82% of patients who get care from both a dermatologist and a rheumatologist have better outcomes than those who see just one. Why? Because skin and joints are two sides of the same immune coin. You need both experts to see the full picture. Regular monitoring matters too. Tools like the MASES score (for enthesitis), Dactylitis Count, and NAPSI (for nail damage) help track progress - not just how you feel, but what’s happening inside.What’s Next?
By 2027, treatment could be guided by your DNA and protein profile. Researchers are already identifying biomarkers that predict who will respond to which drug. The goal? Match the right treatment to the right person - before joint damage starts. And the message is clear: don’t wait. If you have psoriasis and joint pain - even mild stiffness - get checked. Early diagnosis cuts your risk of permanent damage by more than 70%.Frequently Asked Questions
Can psoriatic arthritis develop without skin psoriasis?
Yes. About 15% of people develop joint symptoms before any visible skin changes. This makes diagnosis harder, but if you have a family history of psoriasis, nail changes, or enthesitis, your doctor should still consider psoriatic arthritis.
Is psoriatic arthritis the same as rheumatoid arthritis?
No. Rheumatoid arthritis (RA) typically affects joints symmetrically - both wrists, both knees - and tests positive for rheumatoid factor. Psoriatic arthritis is often asymmetric, doesn’t have that antibody, and includes unique signs like dactylitis, enthesitis, and nail changes. X-rays also show different patterns.
Does psoriatic arthritis affect life expectancy?
Not directly, but uncontrolled inflammation raises your risk of heart disease, stroke, and diabetes. People with PsA have a 2.1-fold higher risk of cardiovascular events. Managing inflammation isn’t just about joints - it’s about your whole body.
Can lifestyle changes help?
Absolutely. Losing weight if you’re overweight reduces joint stress and lowers inflammation. Regular exercise - especially swimming, cycling, or yoga - improves mobility and reduces stiffness. Quitting smoking and limiting alcohol also help. Stress management is critical - it’s one of the top triggers.
Are biologics safe long-term?
Most are, but they require monitoring. TNF inhibitors and IL-17/23 blockers are generally safe for long-term use. JAK inhibitors carry a small increased risk of heart problems and certain cancers, which is why they’re used only after other options fail. Your doctor will weigh risks vs. benefits based on your health history.
Shalini Gautam
February 25, 2026 AT 17:15Finally, someone explains this properly! I’ve had psoriasis since I was 16, and joint pain didn’t show up until I was 28. No one ever connected the dots until my rheumatologist noticed my nail pitting. That’s when everything clicked. My doctor said, ‘Your skin’s been screaming for years-you just didn’t listen.’
And yeah, cold weather? Absolute nightmare. My fingers feel like they’re frozen in cement. I’ve learned to wear gloves even indoors in winter. No one gets it unless they’ve lived it.
Nandini Wagh
February 27, 2026 AT 11:54Oh wow, so the ‘weird nail thing’ wasn’t just me being a weirdo? I thought I was just bad at pedicures. Turns out, my nails were the first warning sign. Classic. Also, ‘psoriatic arthritis’ sounds like a rejected Marvel villain. ‘Behold! I am PsA-the disease that makes your joints look like they lost a fight with a stapler.’
Holley T
March 1, 2026 AT 01:56Okay, but let’s be real-this article is basically a glorified Wikipedia page with extra fluff. You say ‘5 to 10 years before joint pain’-but what’s the actual statistical confidence interval? Did you even check the original studies? And ‘80% have nail changes’? That’s from a 2018 meta-analysis with a sample size of 217. That’s not a population-level finding, that’s a convenience sample.
Also, you mention ‘biologics work in 65%’ but you don’t specify which biologics or what ‘minimal disease activity’ even means. Is that DAS28? MDA? CDAI? No. You just throw numbers around like a TikTok health influencer. This isn’t education-it’s performative simplification.
Dominic Punch
March 1, 2026 AT 13:44You’re not alone. I was misdiagnosed with plantar fasciitis for two years. Turns out? Enthesitis. My heel pain wasn’t from running-it was from my immune system throwing a tantrum. I started walking barefoot on grass every morning. Sounds weird, right? But cold ground + movement = reduced inflammation. Also, turmeric tea. Not a cure. But a daily ritual that helped me feel like I had some control.
And if you’re reading this and you’ve got dactylitis? Please, please, please get an MRI. Don’t wait for X-rays. By then, it’s too late. Your body’s trying to tell you something. Listen.
Valerie Letourneau
March 2, 2026 AT 13:28While I appreciate the comprehensive nature of this exposition, I must express my admiration for the meticulous articulation of clinical phenotypes. The delineation between asymmetric oligoarthritis and distal interphalangeal predominant patterns is particularly salient, as it underscores the necessity for multidisciplinary diagnostic frameworks. In Canada, we have implemented integrated psoriatic disease clinics where dermatologists and rheumatologists co-locate-this model has demonstrably reduced diagnostic latency by 41% in our cohort. I encourage jurisdictions to adopt similar protocols. Health is not siloed; neither should care be.
Khaya Street
March 3, 2026 AT 13:19Look, I’ve got PsA. Been diagnosed 8 years. I’m not mad. Just tired.
Everyone says ‘get checked early.’ But who’s gonna pay for the 12 specialist visits? Who’s gonna take the time off work? My doctor said ‘try methotrexate.’ I did. Made me vomit for three weeks. Then they said ‘try biologics.’ Cost $18K/month before insurance. I’m not rich. I’m not a statistic. I’m a guy who just wants to hold his kid without his hands screaming.
Christina VanOsdol
March 4, 2026 AT 13:52Okay so like, I had a flare last week and I was like 😭😭😭 and then I Googled ‘psoriatic arthritis nail pitting’ and boom-there it was. My nails look like they got into a fight with a cheese grater. And my left knee? Full-on sausage toe vibes. I’m telling you, if you have psoriasis and one weird joint that’s ‘off’-go to a rheum. Like, now. Don’t wait. Don’t ‘wait and see.’ You think you’re being chill? You’re just letting your bones turn into abstract art. 🧠💥🩸
Brooke Exley
March 6, 2026 AT 01:26I want to hug every person who read this far and still feels scared. You’re not broken. You’re not failing. Your body is fighting, and that’s brave.
Here’s what I wish someone told me: It’s okay to grieve the version of yourself that didn’t have joint pain. But don’t let that grief steal your joy. I started swimming three times a week. Water holds you. It doesn’t judge. My hands still ache-but now, I also have laughter, sunrises, and the quiet pride of showing up for myself. You’re not alone. I see you. And you’re doing better than you think.
Alfred Noble
March 7, 2026 AT 02:05