
Imagine waking up in the middle of the night with a pain so sharp and steady in your upper right abdomen that you can't even find a comfortable way to sit or lie down. You might think it's just a bad case of indigestion, but if the pain lasts for hours and doesn't budge regardless of whether you vomit or pass gas, you might be dealing with gallstones. For millions of people, these tiny stones are silent passengers, but when they decide to move, they can turn a normal day into an emergency room visit.
Quick Takeaways
- Biliary Colic: Temporary blockage causing episodic, intense pain.
- Cholecystitis: Serious gallbladder inflammation that requires urgent medical attention.
- The Gold Standard: Laparoscopic cholecystectomy is the preferred surgery for permanent relief.
- Risk Factors: Higher incidence in women and populations with higher obesity rates.
- Timing Matters: Surgery for acute inflammation is most effective when done within 72 hours.
The Mystery of the "Silent" Stones
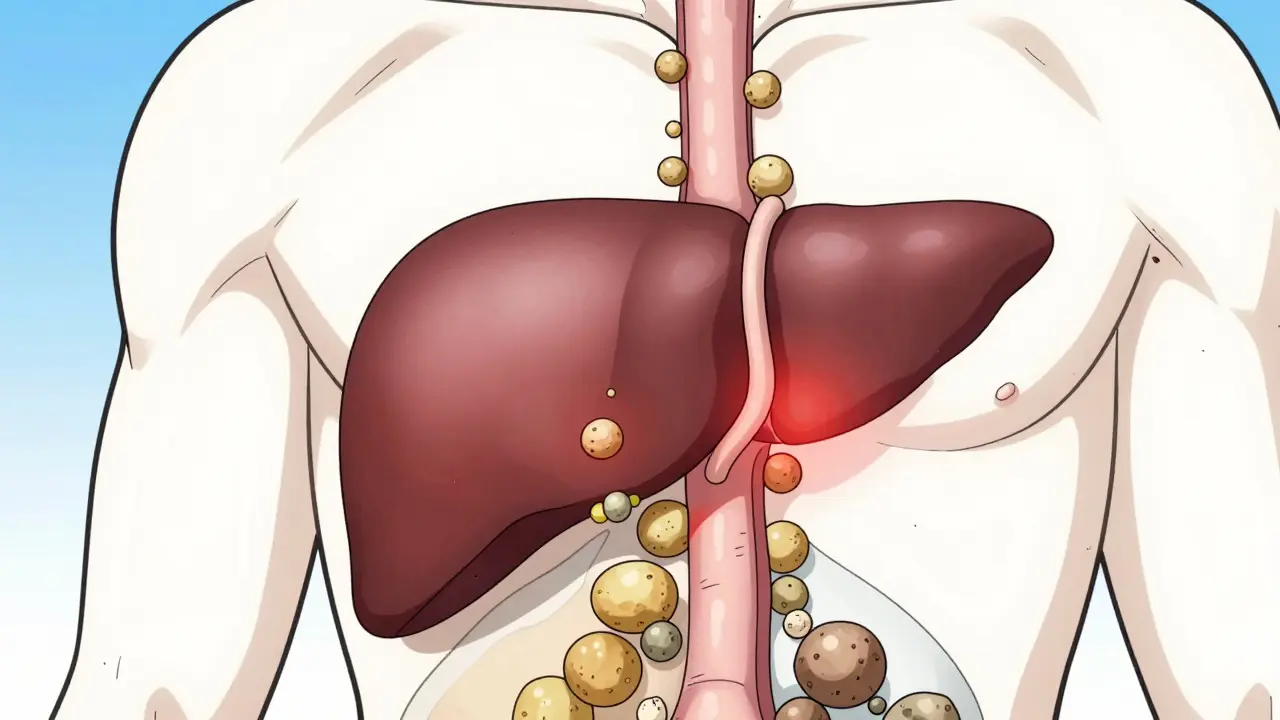
Believe it or not, about 10-15% of adults in developed countries have gallstones. However, most of us will never even know it. About 80% of people with these stones stay asymptomatic their entire lives. But for the unlucky few, the stones migrate. Gallstones is a condition where hardened deposits of digestive fluid collect in the gallbladder. These stones usually come in two flavors: cholesterol stones, which make up 80% of cases in Western countries, and pigment stones, made of bilirubin, which account for the other 20%.
The real trouble starts when a stone decides to take a trip. If a stone blocks the cystic duct-the exit ramp for bile-you experience what doctors call Biliary Colic. This isn't a typical "stomach ache." It's a steady, moderate-to-severe pain localized in the right upper quadrant or the epigastrium. Unlike a gas pain, this doesn't go away with a burp or a bowel movement. It usually peaks within an hour and can last anywhere from one to five hours before the stone shifts and the pressure releases.
When Colic Becomes Cholecystitis
While biliary colic is episodic, it can lead to something far more dangerous. If a gallstone stays stuck in the duct for too long, the trapped bile irritates the gallbladder lining, leading to Cholecystitis. This is effectively an acute inflammation of the gallbladder. While colic is a temporary "traffic jam," cholecystitis is a full-blown medical crisis. About 20% of people who suffer from biliary colic eventually develop this inflammation.
If you aren't careful, the situation can escalate further. A stone might migrate into the common bile duct, causing choledocholithiasis, which often leads to jaundice (yellowing of the skin and eyes). In the worst cases, the obstruction can trigger pancreatitis-a painful and dangerous inflammation of the pancreas. According to NHS data, about 20-30% of people with symptomatic gallstones end up in the hospital within five years of their first attack if they don't get treated.
Comparing Your Treatment Options
If you're staring down a diagnosis of symptomatic gallstones, you generally have three paths: waiting it out, trying medication, or opting for surgery. Let's be honest: waiting it out is a gamble. Research shows that over 90% of people who have one episode of biliary colic will have another within ten years.
For those who can't or won't have surgery, there is ursodeoxycholic acid. It's a medication designed to dissolve small cholesterol stones. While it sounds appealing, it only works in about 30-50% of cases, and half of those people see the stones return within five years. There's also shock-wave lithotripsy, which uses sound waves to break up stones, but this has fallen out of favor because it's mostly effective only for a single, small stone and has a high recurrence rate.
| Method | Effectiveness | Recovery Time | Recurrence Risk |
|---|---|---|---|
| Laparoscopic Surgery | Very High (Gold Standard) | ~7 Days | Very Low |
| Open Surgery | Very High | ~30 Days | Very Low |
| Ursodeoxycholic Acid | Low to Moderate | N/A (Long-term use) | High (50% in 5 years) |
| Shock-wave Lithotripsy | Moderate (Selective) | Quick | High |
The Surgical Path: Laparoscopic vs. Open
When it comes to a permanent fix, the Cholecystectomy (surgical removal of the gallbladder) is the only way to ensure the stones don't come back. Today, 90% of these procedures are performed laparoscopically. Instead of one large incision, the surgeon makes a few tiny holes and uses a camera and specialized tools to remove the organ.
The difference in recovery is night and day. Patients undergoing laparoscopic cholecystectomy usually spend about 1.2 days in the hospital compared to 4.7 days for open surgery. Most people are back to their normal routine in about a week, whereas open surgery can take a month. In experienced hands, the complication rate for the laparoscopic approach is impressively low, often below 2%.
However, surgery isn't a one-size-fits-all solution. For patients over 75 or those with several other health issues, the risks increase. The 30-day mortality rate for a healthy patient is roughly 0.1%, but for those with three or more comorbidities, it can jump to 2.8%. In these high-risk cases, new techniques like endoscopic ultrasound-guided drainage are becoming an alternative for those who can't survive general anesthesia.
What to Expect During and After Recovery
If you are diagnosed with acute cholecystitis, timing is everything. Experts recommend having the surgery within 72 hours. Why? Because waiting too long allows inflammation to build up, which increases the chance that a surgeon will have to "convert" from a laparoscopic approach to a full open surgery. Doing it early drops that conversion rate from 25% down to just 7%.
Post-op care is generally straightforward. Most protocols now emphasize early movement-walking within four hours of waking up-and starting a liquid diet within six hours. Most patients head home within 24 hours. While the majority of people report a massive jump in quality of life, a small percentage (around 18%) experience what's called post-cholecystectomy syndrome. This can include lingering digestive issues or diarrhea, as the body adjusts to how it processes bile without a storage tank.
Living Without a Gallbladder
You might wonder: can I actually live without a gallbladder? Yes. The gallbladder's only job is to store and concentrate bile produced by the liver. Without it, bile just drips continuously into your small intestine. For most, this is a seamless transition. For others, it means being mindful of high-fat meals for a few weeks while the digestive system recalibrates.
If you're feeling the symptoms of biliary colic, don't ignore them. While a single episode might seem manageable, the high likelihood of recurrence and the risk of progressing to cholecystitis make it a condition that requires professional management. Whether it's through the gold-standard laparoscopic cholecystectomy or medical management for high-risk patients, the goal is to stop the cycle of pain before it becomes an emergency.
How do I know if my pain is biliary colic or just gas?
Biliary colic is typically a steady, intense pain in the right upper abdomen that doesn't change when you move, pass gas, or vomit. Gas pain usually shifts, fluctuates, and is often relieved after a bowel movement or burping. If the pain is severe and lasts for several hours, it's more likely to be gallstones.
Is gallbladder surgery a permanent fix?
Yes, a cholecystectomy removes the gallbladder entirely, meaning you can no longer form gallstones within that organ. While some people may develop stones in the common bile duct after surgery, the vast majority of patients experience a total resolution of their biliary colic symptoms.
Can't I just take medication to dissolve the stones?
You can, using drugs like ursodeoxycholic acid, but they are only effective for small cholesterol stones and only in about 30-50% of patients. Furthermore, the recurrence rate is very high-about 50% within five years-making surgery a much more reliable long-term solution.
What are the risks of waiting to have surgery?
The primary risk is that a temporary blockage (colic) turns into permanent inflammation (acute cholecystitis) or blocks the common bile duct. This can lead to jaundice, pancreatitis, or an emergency hospitalization. Since 90% of symptomatic patients will have recurrent pain, waiting often just delays the inevitable surgery while increasing the risk of complications.
Will my diet change after gallbladder removal?
Most people return to a normal diet quickly. However, some may experience temporary diarrhea or bloating after eating very fatty meals because bile is no longer stored and released in large concentrated bursts. Gradually reintroducing fats usually solves this issue.
Next Steps and Troubleshooting
If you are currently in pain: Seek immediate medical attention if your abdominal pain is accompanied by a fever, chills, or yellowing of the skin (jaundice). These are signs of cholecystitis or a bile duct obstruction, which cannot be treated at home.
For those awaiting surgery: Focus on a low-fat diet to avoid triggering another attack. Avoid fried foods, heavy creams, and fatty meats, as these cause the gallbladder to contract, which is what pushes the stone into the duct and causes the pain.
For high-risk patients: If you have severe comorbidities or are over 75, discuss "medical optimization" with your doctor. This involves managing blood pressure and diabetes for 6-8 weeks prior to surgery to reduce the risk of complications.