
Key Takeaways
- FH is a genetic condition causing extremely high "bad" (LDL) cholesterol from birth.
- Early detection through universal and cascade screening is the only way to prevent premature heart attacks.
- Aggressive treatment, often starting in childhood, can normalize life expectancy.
- Genetic testing is the gold standard for diagnosis, though clinical criteria are used more widely.
- Treatment usually requires a combination of high-intensity statins and newer biologics like PCSK9 inhibitors.
Spotting the Warning Signs: Heterozygous vs. Homozygous
Not all cases of FH look the same. It generally falls into two categories: heterozygous (HeFH) and homozygous (HoFH). The difference is mainly about how many "broken" genes you inherited and how severe the symptoms are. Heterozygous FH is the most common form, affecting roughly 1 in 200 to 250 people. For most, there are no outward signs. You feel fine, look fine, and your blood pressure might be normal, but your arteries are silently filling with plaque. Usually, the first "symptom" is a major cardiovascular event before age 50. On the other hand, Homozygous FH is much rarer but far more aggressive. Because the LDL levels are so extreme (often over 400 mg/dL), cholesterol actually leaks out of the blood vessels and deposits into the skin and eyes. You might see xanthomas (waxy cholesterol deposits in the tendons, often the Achilles) or corneal arcus (a white or grey ring around the cornea of the eye). In these cases, heart disease can start in early childhood.The Danger of the "Silent" Phase: Why Early Detection Matters
Why are we pushing for screening in children as young as 9? Because with FH, the damage starts at day one. A typical person's LDL cholesterol rises as they age, but a child with FH has a "cholesterol burden" that accumulates for years before they even hit puberty. If you wait until a standard adult physical to check cholesterol, you've already missed a decade of prevention. The American Heart Association now pushes for universal screening for all children between ages 9 and 11. This isn't about worrying kids about their health; it's about identifying the high-risk few who need immediate intervention to prevent a heart attack in their 30s.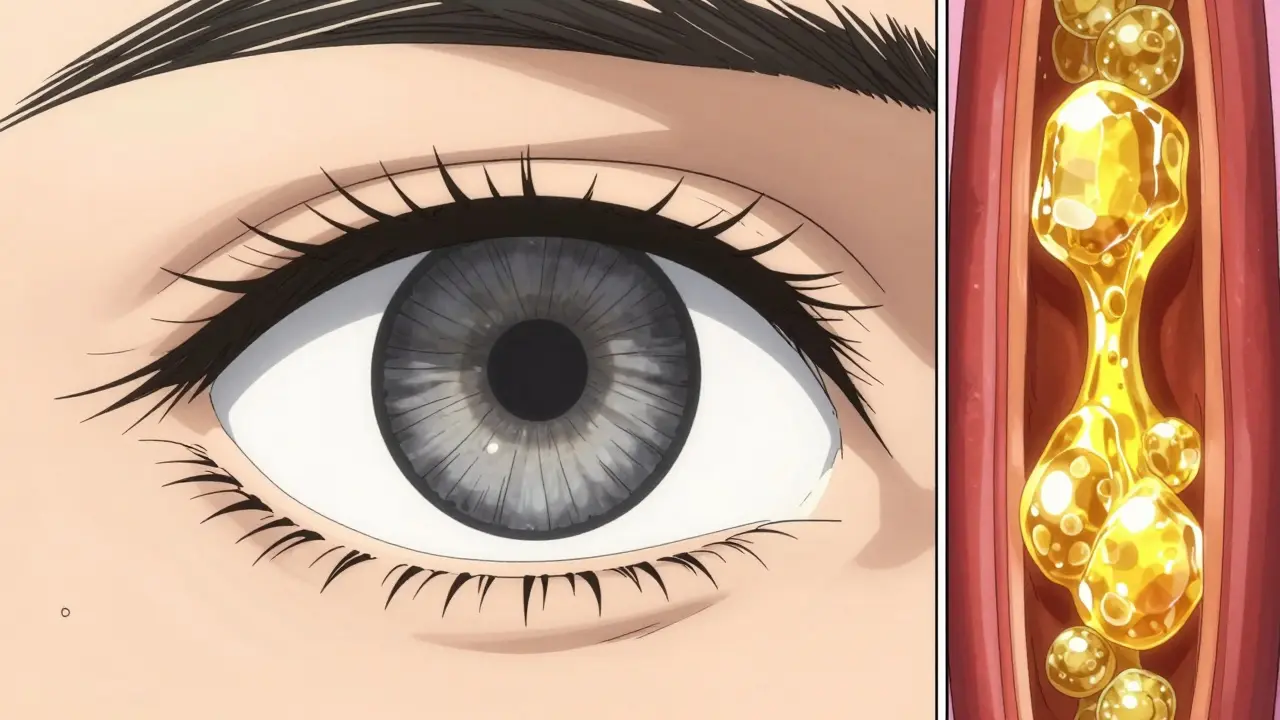
How We Diagnose FH: From Blood Tests to DNA
Diagnosing FH isn't always as simple as one blood test, although that's where it starts. Doctors look at LDL levels-typically, adults with HeFH have LDL over 190 mg/dL, while children are flagged at 160 mg/dL. For the more severe HoFH, that number jumps above 400 mg/dL. When the numbers are high, doctors use clinical tools like the Dutch Lipid Clinic Network (DLCN) criteria, which combine family history, physical signs (like those tendon xanthomas), and lab results to calculate the probability of FH. While these tools are great, the absolute gold standard is Molecular Genetic Testing. This looks for mutations in the LDLR, APOB, or PCSK9 genes. If the test is positive, there is no more guessing. However, because it's expensive, it's not used for everyone-it's usually reserved for confirmed cases and their immediate family members.| Attribute | Heterozygous FH (HeFH) | Homozygous FH (HoFH) |
|---|---|---|
| Prevalence | ~1 in 200-250 people | ~1 in 160,000 to 1 million |
| Typical Adult LDL | > 190 mg/dL | > 400 mg/dL |
| Physical Signs | Often none until heart event | Xanthomas, Corneal Arcus |
| Risk Profile | High (8-10x general pop) | Extreme / Early Childhood |
The Power of Cascade Screening: A Family Affair
If you are diagnosed with FH, you aren't just finding out about your own health-you're potentially saving your children's and siblings' lives. Because FH is an autosomal dominant disorder, there is a 50% chance that any child of an affected parent also has the condition. This leads us to Cascade Screening, which is essentially a targeted search. Instead of screening the whole population, doctors test the first, second, and third-degree relatives of a known patient. It's one of the most cost-effective health interventions in existence. In the Netherlands, this systematic approach has identified over 18,000 cases. In contrast, the US has struggled with implementation, with only a small fraction of eligible families actually getting screened. If you have a diagnosis, the most important "next step" is getting your immediate family tested.
Aggressive Treatment: More Than Just Diet
Let's be clear: you cannot diet your way out of FH. While eating less saturated fat is good for everyone, the underlying genetic defect means your liver simply cannot clear LDL from your blood. You need medical intervention. Statin Therapy is the foundation. These drugs block the enzyme the liver uses to make cholesterol and help lower the amount of LDL in the blood. For many with FH, statins alone aren't enough. They often need a "cocktail" of medications to hit their targets. Modern treatment often adds Ezetimibe, which prevents the gut from absorbing cholesterol, or more powerful biologics like PCSK9 Inhibitors. These are injectable drugs that tell the liver to clear more LDL from the blood. A newer option, inclisiran, is a twice-yearly injection that has made it much easier for patients to stay consistent with their treatment. For those with HeFH, the goal is usually to get LDL below 100 mg/dL. For children, the target is below 135 mg/dL. The key is starting this as early as possible-sometimes as early as age 2 if the risk is high enough.The Future: AI and Automated Detection
We are entering an era where your doctor might not even need to remember to screen you; the computer will do it. New research into Machine Learning algorithms is allowing electronic health records to scan for patterns-age, sex, LDL levels, and family history-to flag potential FH cases automatically. Recent studies show these AI models have a 92% sensitivity rate, far outperforming the manual tools doctors have used for decades. By integrating these tools into every clinic, we can move away from the "accidental discovery" of FH and toward a system of proactive prevention.Can I reverse FH with a plant-based diet?
No. While a healthy diet helps overall heart health, FH is a genetic mutation. Your liver is physically unable to process LDL cholesterol efficiently. Medication is required to lower levels to a safe range and prevent heart attacks.
When should my children be tested for FH?
The American Heart Association recommends universal screening for all children between ages 9 and 11. However, if a parent is already diagnosed with FH, testing may be recommended as early as age 2 to start preventative treatment.
Is genetic testing necessary for a diagnosis?
It is the gold standard and provides the most definitive answer. However, doctors can often make a clinical diagnosis using the Dutch Lipid Clinic Network (DLCN) criteria based on LDL levels and family history if genetic testing is too expensive or unavailable.
What are the most effective medications for FH?
High-intensity statins are the first line of defense. If targets aren't met, doctors typically add ezetimibe or PCSK9 inhibitors (like inclisiran) to aggressively bring LDL levels down.
What is cascade screening?
Cascade screening is the process of testing the biological relatives (parents, siblings, and children) of a person diagnosed with FH. Because it's a dominant genetic trait, there's a 50% chance relatives are also affected.