
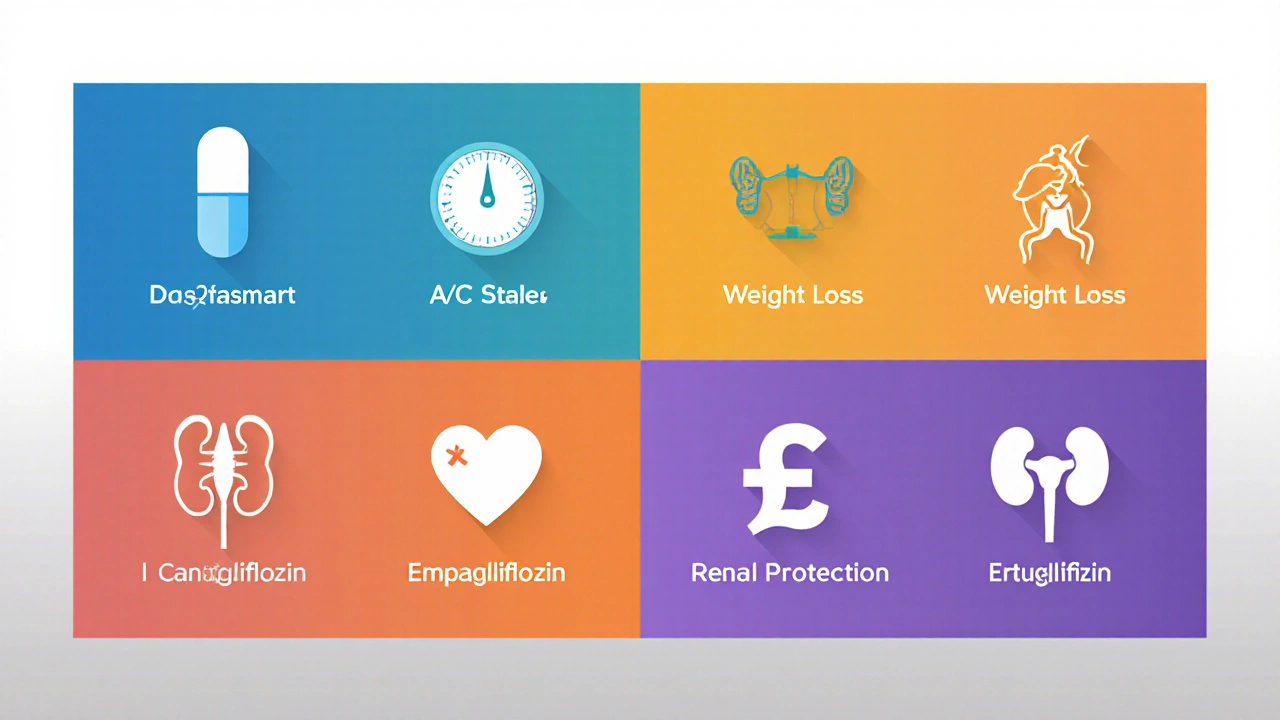
Dapasmart vs Alternatives Comparison Tool
Dapasmart
- A1C Reduction 0.6-0.9%
- Weight Loss 2-3 kg
- CV Benefit 14%
- Kidney Benefit 28%
- Cost $580/year
Canagliflozin
- A1C Reduction 0.5-0.8%
- Weight Loss 2-4 kg
- CV Benefit 12%
- Kidney Benefit 25%
- Cost $610/year
Empagliflozin
- A1C Reduction 0.6-0.9%
- Weight Loss 3-4 kg
- CV Benefit 17%
- Kidney Benefit 30%
- Cost $590/year
Ertugliflozin
- A1C Reduction 0.5-0.8%
- Weight Loss 2-3 kg
- CV Benefit 13%
- Kidney Benefit 27%
- Cost $620/year
Decision Factors
Clinical Benefits
- Empagliflozin: Strongest cardiovascular outcomes
- Dapasmart: Good balance of efficacy and safety
- Canagliflozin: Higher amputation risk
- Ertugliflozin: Newer with limited long-term data
Practical Considerations
- Cost: Dapasmart ($580) is competitive
- Side Effects: UTIs common across all
- Contraindications: Avoid in eGFR < 30 mL/min
- Generic Availability: Dapagliflozin generics now available
Important Note
Always consult your healthcare provider before switching medications. Individual factors such as kidney function, history of infections, and other medical conditions affect suitability.
Key Takeaways
- Dapasmart (dapagliflozin) offers strong glucose‑lowering and heart‑protective benefits.
- Canagliflozin, empagliflozin and ertugliflozin share the same class but differ in dosing, side‑effect profiles, and FDA‑approved indications.
- Metformin remains the backbone therapy; adding an SGLT2 inhibitor like Dapasmart is usually for patients needing extra A1C reduction or cardiovascular protection.
- Cost, insurance coverage, and kidney function are the biggest practical factors when picking an alternative.
- Talk to your clinician about personal risk factors-especially history of urinary infections or low blood pressure-before switching.
When it comes to managing type 2 diabetes, the market is crowded with options that promise lower blood sugar, weight loss, and heart health. Dapasmart is the branded version of dapagliflozin, a sodium‑glucose co‑transporter‑2 (SGLT2) inhibitor approved for adults with type 2 diabetes, heart failure, and chronic kidney disease. If you’re reading this, you’re probably wondering how it stacks up against other pills you’ve heard about. Below we break down the most common alternatives, walk through the numbers that matter, and give you a quick decision‑making guide.
How Dapasmart Works
Dapasmart belongs to the SGLT2 inhibitor class, which works by blocking the SGLT2 protein in the kidney’s proximal tubules. This prevents glucose from being re‑absorbed into the bloodstream, forcing the body to excrete excess sugar in the urine. The result is a modest A1C drop (about 0.6‑0.9%) along with a typical weight loss of 2‑3kg and a reduction in systolic blood pressure by 3‑5mmHg.
The standard dose is 10mg once daily, taken with or without food. For patients with moderate kidney impairment (eGFR≥30mL/min/1.73m²), the dose can be lowered to 5mg, but the drug is not recommended below that threshold.
What the Alternatives Are
Within the SGLT2 family, three other FDA‑approved drugs compete directly with dapagliflozin:
- Canagliflozin - marketed as Invokana, typically dosed at 100mg or 300mg daily.
- Empagliflozin - sold as Jardiance, available in 10mg and 25mg tablets.
- Ertugliflozin - known as Steglatro, offered in 5mg and 15mg doses.
Beyond the SGLT2 class, the most common background therapy is Metformin - a biguanide that improves insulin sensitivity and is usually the first‑line drug. For patients who need additional control, clinicians may add a GLP‑1 receptor agonist such as Liraglutide (Victoza) or other injectable options.
Side‑Effect Landscape
All SGLT2 inhibitors share a core set of side effects: genital mycotic infections, urinary tract infections, and mild dehydration. However, each molecule has unique nuances.
- Dapasmart - lowest reported rates of lower‑limb amputations; modest increase in ketoacidosis risk in patients with low carbohydrate intake.
- Canagliflozin - higher signal for amputations and bone fractures, especially at the 300mg dose; still strong cardiovascular benefit.
- Empagliflozin - excellent heart‑failure outcomes; slightly higher incidence of mild hypotension.
- Ertugliflozin - newer on the market, similar safety to dapagliflozin but limited long‑term data.
Metformin’s most common issue is gastrointestinal upset (nausea, diarrhea), which can often be mitigated by dose titration or using an extended‑release formulation.
How They Compare on the Numbers
| Metric | Dapasmart (dapagliflozin) | Canagliflozin | Empagliflozin | Ertugliflozin | Metformin |
|---|---|---|---|---|---|
| A1C reduction | 0.6‑0.9% | 0.5‑0.8% | 0.6‑0.9% | 0.5‑0.8% | 1.0‑1.5% |
| Weight loss | 2‑3kg | 2‑4kg | 3‑4kg | 2‑3kg | 0‑1kg (neutral) |
| Cardiovascular benefit (MACE reduction) | 14% | 12% | 17% | 13% | Neutral |
| Kidney disease progression slowdown | 28% | 25% | 30% | 27% | Modest (10‑15%) |
| Annual wholesale cost (US, 2024) | $580 | $610 | $590 | $620 | $30 (generic) |
| Common side‑effects | UTI, genital yeast | UTI, amputations (high dose) | UTI, mild hypotension | UTI, limited data | GI upset |
Choosing the Right Option - Decision Checklist
- Cardiovascular risk - If heart failure or prior MACE is a concern, empagliflozin has the strongest data, followed closely by Dapasmart.
- Kidney function - All SGLT2 inhibitors are effective down to eGFR30mL/min, but dapagliflozin and empagliflozin have the most robust renal outcome studies.
- Amputation risk - Avoid canagliflozin if you have peripheral arterial disease or a history of foot ulcers.
- Cost/insurance - Generic metformin remains cheapest; many plans cover branded SGLT2 inhibitors at similar co‑pay levels, but check tier‑specific pricing.
- Side‑effect tolerance - Patients prone to yeast infections may prefer ertugliflozin (newer, slightly lower infection rates) or a lower dose of dapagliflozin.
Potential Pitfalls and How to Avoid Them
Switching between SGLT2 inhibitors is generally safe, but keep an eye on three red flags:
- Dehydration - Increase water intake, especially if you’re on a diuretic or live in a hot climate.
- Ketoacidosis - Rare but serious; monitor for nausea, abdominal pain, or rapid breathing, and avoid extreme low‑carb diets while on the medication.
- Drug interactions - Combining SGLT2 inhibitors with loop diuretics can amplify blood‑pressure drops. Review any new prescriptions with your pharmacist.
Real‑World Example
Maria, a 62‑year‑old with a 10‑year history of type 2 diabetes, hypertension, and stage 3 chronic kidney disease (eGFR45), was on metformin 1000mg BID. Her A1C plateaued at 8.2% and she recently had a mild heart‑failure episode. Her cardiologist added Dapasmart 10mg daily. Six months later, her A1C fell to 7.3%, she lost 3kg, and her NYHA class improved from II to I. She experienced a single episode of a mild vaginal yeast infection, which resolved with a short antifungal course. If Maria had peripheral artery disease, her doctor might have chosen empagliflozin instead to avoid the very low amputation risk associated with canagliflozin.
Bottom Line
If you need an add‑on to metformin that also protects your heart and kidneys, Dapasmart vs alternatives leans in favor of dapagliflozin for most patients without high amputation risk. It balances efficacy, safety, and cost better than canagliflozin, while offering comparable outcomes to empagliflozin. Always let your healthcare provider weigh your personal health profile against these data points before making a switch.

Frequently Asked Questions
Can I take Dapasmart with insulin?
Yes, dapagliflozin can be combined with basal or bolus insulin. The drug works by eliminating glucose in the urine, a mechanism independent of insulin, so they complement each other. Watch for a higher risk of hypoglycemia if your insulin dose isn’t adjusted.
What if my eGFR drops below 30mL/min?
Dapasmart is not recommended when eGFR is under 30mL/min/1.73m² because the kidney can’t filter glucose effectively, reducing the drug’s benefit and increasing side‑effects. Your doctor may switch you to a non‑SGLT2 agent like a DPP‑4 inhibitor.
Is there a generic version of dapagliflozin?
As of 2025, generic dapagliflozin is available in the US and Europe, priced around $450 annually. Check your pharmacy’s formulary; sometimes the brand Dapasmart has a lower co‑pay due to manufacturer discounts.
Do SGLT2 inhibitors cause weight gain?
No, they usually cause modest weight loss because the body loses calories through glucose excretion. Most users report losing 2‑4kg after three to six months of therapy.
How do I know if I’m having a urinary tract infection?
Typical signs include burning during urination, cloudy or foul‑smelling urine, and a frequent urge to go. If you notice any of these, contact your clinician promptly; early treatment can prevent complications.
Alan Kogosowski
October 3, 2025 AT 18:50When you look at the data presented for dapagliflozin, marketed here as Dapasmart, the first thing that jumps out is the balance of efficacy and safety across multiple endpoints, which is something that many clinicians find reassuring in an era of ever‑increasing therapeutic options. The A1C reduction of 0.6‑0.9% sits comfortably alongside the weight loss of roughly 2‑3 kg, making it comparable to the higher‑dose canagliflozin but without the attendant amputation warnings that have haunted that molecule for years. Cardiovascular benefit, quantified at a 14% reduction in major adverse cardiovascular events, is slightly lower than empagliflozin’s 17% but still clinically meaningful, especially for patients who do not tolerate higher‑dose agents. The renal protection numbers – a 28% slowdown in disease progression – also outpace both canagliflozin and ertugliflozin, positioning dapagliflozin as a versatile choice for patients with moderate kidney impairment. From a pharmacoeconomic perspective, the annual cost of $580 places it under the other branded agents, which often exceed $600, and it now faces competition from generics that further lower the barrier to access. In practice, the tolerability profile is favorable; the incidence of genital mycotic infections remains comparable to its class peers, but the lower risk of severe hypoglycemia when combined with metformin makes it a safe add‑on for many patients. It’s also worth noting that the drug does not require dose adjustments for most patients with an eGFR down to 30 mL/min, whereas some alternatives lose efficacy or require tighter monitoring in that range. The lack of a significant diuretic effect beyond modest reductions in systolic blood pressure means that clinicians can combine dapagliflozin with loop diuretics without fearing excessive volume depletion. Real‑world evidence, like the case of Maria cited in the article, underscores that the theoretical benefits translate into tangible outcomes such as a 0.9 % drop in A1C, modest weight loss, and improvement in heart‑failure class. Compared with empagliflozin, the difference in cardiovascular benefit may be marginal for patients whose primary concern is heart failure, but the cost advantage and generic availability often tip the scales in favor of dapagliflozin. Conversely, patients with a history of peripheral arterial disease might still favor empagliflozin due to its slightly lower amputation risk profile. Ultimately, when you synthesize the efficacy, safety, cost, and formulary considerations, dapagliflozin emerges as the most balanced SGLT2 inhibitor for the average type‑2 diabetic patient who does not have specific contraindications or extremely high cardiovascular risk.
Ben Lee
October 5, 2025 AT 00:46I totally agree with the deep dive you just gave, it really helps to see the numbers laid out in plain language. From a practical standpoint, I’ve seen patients who switch from canagliflozin to dapagliflozin and notice fewer foot‑related complications, which aligns with the lower amputation signal you mentioned. The cost difference, although not massive, does matter for those on a fixed income, especially when generic dapagliflozin becomes more widely available.
David Brice
October 6, 2025 AT 06:46Hey folks, just wanted to add some extra context. If you aren't already on metformin, start there because it gives you the biggest A1C drop (1‑1.5%). Then think about dapagliflozin as your next step if you need extra cardio‑renal protection. Also, watch out for UTIs – I've seen a few patients get them after a month on any SGLT2. Keep your water intake up! Lastly, if your eGFR falls under 30, consider switching to a DPP‑4 inhibitor instead – they’re easier on the kidneys.
Zachary Schroer
October 7, 2025 AT 12:46Really? Everyone’s blowing up dapasmart like it’s the holy grail. Sure, it’s decent but empagliflozin still reigns supreme on CV outcomes. 🙄💁♂️
Stacy Whitman
October 8, 2025 AT 18:46American patients deserve the best – Dapasmart is clearly superior.
Mina Berens
October 10, 2025 AT 00:46🤔 interesting take! I still think each drug has its place – it really depends on the individual patient’s profile 😊
Chris Meredith
October 11, 2025 AT 06:46Yo fam, let’s break it down fast: dapagliflozin gives you decent glucose control, moderate weight loss, and solid kidney benefits – all without the pricey hype. The jargon‑heavy part is the eGFR threshold; if you’re above 30, you’re good. If you want to talk cost‑efficiency, dapagliflozin’s generic hit the market and now you’re looking at $450 a year, which is a sweet spot for most health plans.
Jessie Eerens
October 12, 2025 AT 12:46Consider, for a moment, the philosophical implications of pharmaceutical choice: does one prioritize marginally higher cardiovascular benefit (as with empagliflozin) over cost‑effectiveness (as with generic dapagliflozin)? The answer, of course, lies not merely in numbers but in the lived experience of the patient; thus, the clinician must weigh not only the statistical significance but also the existential quality of life-something that no randomized controlled trial can fully capture.
Caroline Lane
October 13, 2025 AT 18:46Seriously, why are we even debating? People just need a pill and they’re fine.
Geneva Lyra
October 15, 2025 AT 00:46Hey there! Just wanted to share that I’ve seen many of my patients feel more comfortable with dapagliflozin because the generic version really reduces out‑of‑pocket costs, plus the side‑effect profile is pretty manageable. A quick tip: always remind them to stay hydrated, especially if they’re also on a diuretic.
Ellie Haynal
October 16, 2025 AT 06:46Wow, the drama around SGLT‑2 inhibitors never ends. Some say dapagliflozin is the underdog hero, others scream about empagliflozin’s superiority. Either way, the real story is how many patients end up battling side‑effects like yeast infections while doctors fight over market share. It’s exhausting.
Jimmy Gammell
October 17, 2025 AT 12:46👍 Totally get that! If you’re juggling multiple meds, dapagliflozin’s once‑daily dosing makes life easier. And yes, keep an eye on those UTIs – a quick check‑up can save a lot of hassle later. 😊