
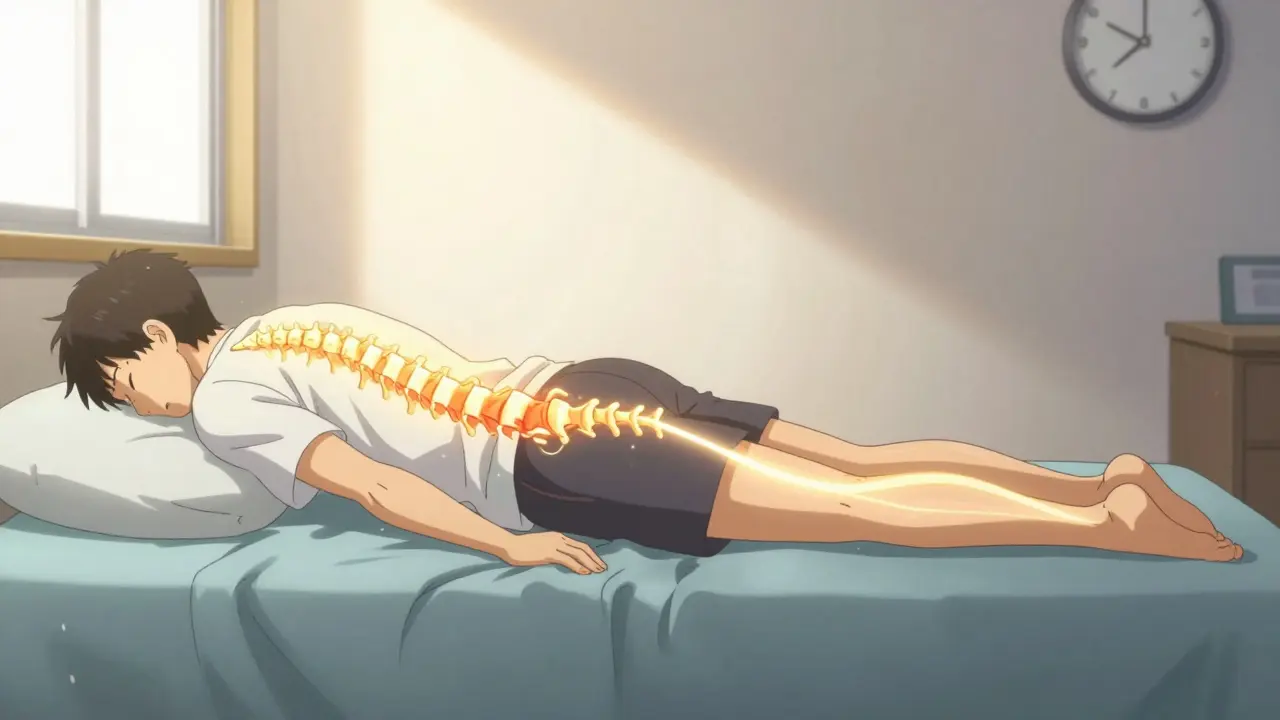
When your neck or lower back sends sharp, shooting pain down your arm or leg, it’s not just a bad ache-it’s your nerve screaming for help. This is radiculopathy, and it’s more common than you think. About 1 in 5 adults will deal with it at some point, especially if you’re between 45 and 64. The pain doesn’t come from the spot you feel it. It’s coming from a pinched nerve in your spine. Cervical radiculopathy hits the neck area, and lumbar radiculopathy-often called sciatica-strikes the lower back. Both are nerve problems, not muscle problems. And if you treat them like muscle strains, you’ll waste months and make things worse.
What’s Really Happening Inside Your Spine?
Your spinal nerves branch out like roots from a tree. When something squishes or irritates those roots, you get pain, numbness, or weakness in the area they serve. It’s not magic-it’s anatomy. For cervical radiculopathy, the problem usually starts with a slipped disc or bone spur pressing on a nerve root in your neck. The most common offenders? C6 and C7 nerves. If C6 is pinched, you’ll feel pain from your shoulder down to your thumb and index finger. You might even notice your biceps getting weak. If C7 is affected, the pain runs down to your middle finger, and your triceps might feel like they’ve lost power.
Lumbar radiculopathy works the same way but in your lower back. L5 and S1 nerves are the usual suspects. L5 pinching means pain shoots down the outside of your calf to your big toe. You might catch your foot dragging when you walk. S1 irritation? That’s classic sciatica: pain from your butt down the back of your leg to the sole of your foot, with weak ankle movement. These aren’t random pains. They follow exact maps called dermatomes. If your doctor doesn’t ask about where the pain travels, they’re not looking at the real issue.
Why Some People Get It and Others Don’t
It’s not just aging. People under 50 usually get radiculopathy from a sudden disc herniation-like when you lift something heavy wrong or twist too fast. But after 50, it’s mostly degeneration. Bone spurs grow. Discs flatten. The space where nerves exit gets narrower. That’s why older adults get it more often. Men are slightly more likely to get lumbar radiculopathy-probably because of jobs involving heavy lifting. Cervical radiculopathy? It’s almost even between men and women.
Work matters. Construction workers, nurses, and warehouse staff have over three times the risk. Sitting all day? That’s not the main cause, but poor posture while sitting can make it worse. And yes, trauma plays a role. About 1 in 5 cervical cases start after a car accident or fall. That’s way higher than in the lower back.
Most People Get Better Without Surgery
Here’s the good news: 85% of people with radiculopathy get better in 12 weeks without surgery. That’s not a guess-it’s from large studies. But “better” doesn’t mean “ignore it.” Passive rest won’t fix it. You need the right kind of movement. The first step is always conservative care: activity changes, anti-inflammatory meds like ibuprofen, and physical therapy.
Medications help with inflammation and pain, but they don’t fix the root problem. Physical therapy does. A 2021 study found that 68% of people had major symptom reduction with PT, compared to just 52% with meds alone. That’s a big gap. The key is timing. The American College of Physicians says wait 6 to 8 weeks before jumping to injections or surgery. Rushing into an epidural shot? It might give you temporary relief, but studies show no lasting benefit beyond 6 weeks. And for some, it doesn’t help at all.
How Rehabilitation Actually Works
Rehab isn’t one-size-fits-all. The best programs are built around your specific nerve problem.
For cervical radiculopathy:
- Weeks 1-2: Cut back on heavy lifting, avoid looking down at your phone for long periods. Use a supportive pillow. Try gentle neck stretches and chin tucks.
- Weeks 2-4: Add cervical traction-light pull (5-10 lbs) for 10-15 minutes daily. This opens up space around the nerve.
- Weeks 4-8: Start isometric exercises. Push your hand against your forehead without moving your head. Hold for 5 seconds. Repeat 10 times. This strengthens without stressing the nerve.
- Weeks 8-12: Move to dynamic stability. Scapular retractions (squeezing shoulder blades together) and light resistance band rows help support your neck long-term.
For lumbar radiculopathy:
- Weeks 1-2: Avoid bending or twisting. Sleep on your side with a pillow between your knees. Try lying on your stomach for 5-10 minutes a day-this gently stretches the lower spine.
- Weeks 2-4: Begin McKenzie extension exercises. Lie on your stomach, prop yourself up on your elbows, then slowly lift your chest. Hold for 5 seconds. Repeat 10 times, twice a day.
- Weeks 4-8: Focus on core stability. Dead bugs, bird-dogs, and glute bridges build the muscles that protect your spine. No sit-ups. They crush the discs.
- Weeks 8-16: Add functional movement. Practice standing up from a chair without using your hands. Walk daily. Progress slowly.
Most people need 12 to 16 PT sessions to get real results. And the biggest factor in success? Doing the exercises at home. People who stick to their routine recover 47% faster than those who don’t.
The Hidden Pitfalls
Too many people make the same mistakes-and they cost them time and pain.
- Returning to heavy lifting too soon: 28% of people who go back to lifting before their spine is ready end up with the same pain again.
- Skipping home exercises: 61% of people who don’t improve admit they never did their exercises consistently.
- Using bad pillows: A pillow that’s too flat or too high keeps your neck twisted. Use one that keeps your head in line with your spine.
- Ignoring ergonomics: If you work at a desk, raising your monitor to eye level cuts neck strain by 32%. Adjust your chair so your feet are flat and your knees are at 90 degrees.
And don’t fall for the quick-fix myth. Epidural injections? They’re not magic. Some patients swear by them, but studies show they don’t change long-term outcomes. If you’re still in pain after 12 weeks, it’s not because you didn’t try hard enough-it’s because the approach wasn’t right.
What’s New in Treatment?
There’s exciting progress. In early 2023, the FDA approved the first AI tool that analyzes MRI scans to find nerve compression with 96.7% accuracy-up from 89%. That means faster, more precise diagnoses.
Researchers are now testing personalized rehab plans based on exactly which nerve is affected. Early results show 41% better movement recovery than standard programs. There’s also early work with targeted steroid nanoparticles and platelet-rich plasma (PRP) injections. But PRP isn’t proven yet. Don’t pay thousands for it until more data comes in.
What to Expect Long-Term
Most people get their life back. Within a year, 82% return to their normal activities. Only 8% end up with chronic pain. That’s not a guarantee-it’s a pattern. The difference? Early, consistent rehab. People who wait, ignore symptoms, or rely on painkillers alone are the ones who get stuck.
Recovery isn’t about being pain-free overnight. It’s about rebuilding strength, movement, and confidence. It’s about learning how your body works so you don’t break it again. And if you’re one of the 15% who don’t improve? That’s when you need a specialist who looks beyond the X-ray-someone who listens to your story, not just your scan.
Can radiculopathy go away on its own without treatment?
Yes, in most cases. About 85% of people with cervical or lumbar radiculopathy see major improvement within 12 weeks without surgery. But “on its own” doesn’t mean doing nothing. Resting completely, avoiding aggravating movements, and using basic pain relief like NSAIDs are part of the process. Skipping movement entirely, however, can lead to stiffness and slower healing. Active recovery-like gentle stretching and walking-is what helps the body heal faster.
Is surgery necessary for radiculopathy?
Surgery is rarely the first option. Only about 15% of cases need it. Surgeons recommend it when there’s clear nerve damage-like muscle weakness that’s getting worse, loss of bladder or bowel control (cauda equina syndrome), or if conservative treatment fails after 6 to 12 weeks. Most people recover with physical therapy, activity changes, and time. Surgery carries risks and a long recovery. It’s not a shortcut-it’s a last resort for specific situations.
Why does my pain travel down my arm or leg?
Because nerves don’t stop at the spine. The nerve root that’s pinched in your neck or lower back runs all the way down your arm or leg. When it’s irritated, the pain signal travels along that path. That’s why a disc problem in your neck can make your hand numb, or a lower back issue can cause foot pain. It’s not the hand or foot that’s broken-it’s the nerve signal being disrupted upstream.
Can I still exercise with radiculopathy?
Yes-but not all exercise. Avoid heavy lifting, twisting, or high-impact activities like running or jumping until symptoms improve. Low-impact movement like walking, swimming, or stationary cycling is safe and actually helps reduce inflammation. Specific rehab exercises, like chin tucks for neck pain or bird-dogs for lower back pain, are designed to strengthen without irritating the nerve. Always start slow and stop if pain shoots down your limb.
Do epidural steroid injections cure radiculopathy?
No. Epidural injections can reduce inflammation and give temporary pain relief-usually for 2 to 6 weeks. But they don’t fix the cause, like a herniated disc or bone spur. Studies show no long-term benefit compared to placebo. Some people feel better after an injection, but that doesn’t mean the nerve healed. They’re a tool to help you get through a tough patch so you can do rehab. Don’t rely on them as a cure.
How long does physical therapy take to work?
Most people start noticing improvement in 3 to 6 weeks, but full recovery often takes 12 to 16 weeks. This is because healing nerves and rebuilding muscle strength takes time. The key isn’t how many sessions you attend-it’s how consistently you do your home exercises. People who stick to their routine recover nearly twice as fast. If you’re not seeing progress after 8 weeks, ask your therapist to adjust your program. Not all exercises work for everyone.
Can poor posture cause radiculopathy?
Not directly, but it can make it much worse. Poor posture doesn’t usually cause a disc to herniate, but it increases pressure on your spine over time. Slouching at a desk, holding your phone to your ear, or sleeping with your neck twisted can irritate already sensitive nerves. Correcting posture doesn’t cure radiculopathy, but it removes a major aggravating factor. Simple fixes-like raising your monitor or using a supportive pillow-can reduce symptoms by over 30%.
Is radiculopathy the same as sciatica?
Sciatica is a type of radiculopathy. Radiculopathy is the umbrella term for any nerve root irritation in the spine. Sciatica specifically refers to pain from the S1 or L5 nerve roots in the lower back that travels down the leg. So all sciatica is radiculopathy, but not all radiculopathy is sciatica. Cervical radiculopathy affects the neck and arms. Sciatica affects the lower back and legs. They’re related but different.
What Comes Next
If you’re dealing with this right now, your next step isn’t another scan or another shot. It’s consistency. Start with the right rehab exercises for your area-neck or lower back. Do them every day, even if you feel better. Adjust your workspace. Sleep with proper support. Avoid sudden movements. Track your progress. If pain doesn’t improve in 4 weeks, find a physical therapist who specializes in spine rehab-not just general fitness.
The body heals best when you work with it, not against it. Radiculopathy isn’t a life sentence. It’s a signal. Listen to it. And act smart.
Lorna Brown
March 13, 2026 AT 20:14What really struck me is how radiculopathy isn’t just a physical issue-it’s a communication breakdown between your spine and your nervous system. The body’s not broken, it’s screaming for attention. I’ve seen people treat this like a muscle strain and wonder why nothing works. It’s not about strength, it’s about alignment. And the dermatome maps? That’s pure anatomy poetry. If your doc doesn’t map your pain like a topographic chart, you’re being mismanaged.
Also, the 85% recovery stat without surgery? That’s not luck. That’s the body’s innate wisdom when you stop fighting it and start listening. We’ve been sold a myth that pain = damage. But pain is just data. The real work is in decoding it.
Rex Regum
March 14, 2026 AT 10:11Oh great, another ‘physical therapy is magic’ post. Let me guess-next you’ll tell me yoga cures cancer? I’ve had lumbar radiculopathy for 14 months. Did your ‘68% improvement with PT’ stat include people who did PT for 6 months and still couldn’t walk without screaming? Nah. And don’t even get me started on those ‘gentle stretches’-I’ve done every damn one. They’re not magic. They’re placebo with a price tag.
Meanwhile, my surgeon says I’ve got a herniated L5-S1 with nerve root compression. No amount of chin tucks is gonna fix that. You’re giving people false hope while real cases get ignored. Thanks for the pseudoscience.
Kelsey Vonk
March 14, 2026 AT 13:48Thank you for this 💙 I’ve been dealing with cervical radiculopathy since last winter and this is the first time I’ve seen someone explain it without jargon or fear tactics. The part about the pillow? Game changer. I was using this fluffy one that felt nice but made my neck twist all night. Switched to a medium-firm one and the numbness in my thumb? Gone in 3 days.
Also, I did the chin tucks and cervical traction for 3 weeks straight and didn’t even think it was working… until one morning I could turn my head without wincing. Turns out healing is quiet. You don’t feel it until you’re already better. So proud of myself for sticking with it 😊
Emma Nicolls
March 15, 2026 AT 20:31OMG I finally get it why my arm goes numb when I scroll too long 😭 I thought it was just carpal tunnel but nooo it’s my C6 nerve getting squished from looking down at my phone all day
just started the chin tucks and im already feeling better like 2 days in?? like i dont even need meds anymore??
also my pillow was trash i switched to this one from amazon and its a dream
thank you thank you thank you
Jimmy V
March 17, 2026 AT 18:55Stop. Just stop. This isn’t a self-help blog. You’re not ‘listening to your body’-you’re managing a biomechanical compression. The 85% recovery stat? That’s for mild cases with no neurological deficit. If you have foot drop or hand weakness, you’re not getting better with ‘gentle stretches.’
PT works because it reduces inflammation and restores mobility-not because it’s ‘spiritual.’ And yes, epidurals don’t cure it. But they buy time for rehab to work. You’re conflating treatment with cure. Don’t be a hero. See a spine specialist before you turn your sciatica into a lifestyle blog.
Richard Harris
March 18, 2026 AT 18:28Interesting read, very thorough. I’ve had lumbar radiculopathy for over two years now, mostly from years of warehouse work. The exercises you listed are spot on, especially the bird-dogs and dead bugs. I started them six months ago and honestly, I didn’t believe they’d help-but now I can lift my grandkids without pain.
One thing I’d add: sleep position matters more than people think. Side sleeping with a pillow between the knees? Absolute game-changer. I wish someone had told me that years ago.
Kandace Bennett
March 20, 2026 AT 11:45OMG I’m so glad someone finally got it right!! 🙌 I’m a physical therapist in Austin and I see people come in with 3 different sets of ‘rehab’ advice from TikTok every week. This? This is what actual science looks like. No fluff. No fake cures. Just anatomy, timing, and consistency.
And can we talk about how people pay $2,000 for PRP injections and then cry because it didn’t work? Honey, you’re not a unicorn. Your body doesn’t need magic. It needs 12 weeks of bird-dogs and a pillow that doesn’t look like a marshmallow.
Also, if you’re still using your iPhone in bed? Stop. You’re not a child. You’re an adult with a spine. 🥵
Tim Schulz
March 21, 2026 AT 16:23Wow. Just… wow. The way this post casually drops ‘FDA-approved AI tool with 96.7% accuracy’ like it’s a new iPhone feature? I’m impressed. And then you follow it up with ‘don’t pay for PRP until more data comes in’-as if anyone with a credit card and a YouTube subscription hasn’t already blown $5K on ‘nerve-rejuvenating’ serums.
Meanwhile, I’m over here with a herniated disc and a 401(k) that’s now 12% PT sessions. The real tragedy? The system rewards the people who do nothing, not the ones who show up every day for bird-dogs.
Also, if you think ‘consistency’ is the secret, you’ve never met my cat. She sits on my back while I do stretches. That’s not rehab. That’s a hostage situation. 😅